 Armand Halbert
Software Engineer
Contact:
armand.halbert@gmail.com
Armand Halbert
Software Engineer
Contact:
armand.halbert@gmail.com
Cribsheet
Cribsheet: A Data-Driven Guide to Better, More Relaxed Parenting, from Birth to Preschool. By Emily Oster, PhD. 326 pages.
Mommy forums are full of arguments about what is right and wrong for your child. What should your policy be for screen time? What’s the best way to approach potty training? Most of these arguments are based around ancedata. Worse, they often come with a lot of judgment attached to them. If you sleep train your baby, you don’t care about them at all.
Cribsheet is the answer to all this. This is the second book in economist Emily Oster’s Parentdata series. Like the first entry, Expecting Better, Dr. Oster takes a look at the data on a broad swath of parenting controversies and distills it into non-judgmental advice on how to raise your little one. Some of it will be controversial, such as her advice on breastfeeding: marginally better for your child’s health than formula, but no need to kill yourself over it. On other topics, like vaccines, she follows the conventional wisdom.
More often than not, though, the data is inconclusive - a parental choice is neither good nor bad. In that case, Dr. Oster suggests that you do what works for your family. That will frustrate parents looking for explicit guidelines, but I found it relaxing to know many of the choices we agonize over will not matter too much.
That, of course, still means you have to find something that works for your family. Alongside her research, Dr. Oster presents common microeconomic concepts to help you make better choices, from decision trees to Bayesian reasoning. I found these parts too simplified to be really helpful, but I imagine the book would not have sold well if it became a treatise on decision theory.
There are limits to the kind of economic thinking espoused by the book. Much of the advice offered in the book only matters if you have some degree of economic flexibility. Take the chapter on childcare. Dr. Oster only considers having a nanny vs. daycare. Given that only 37% of children under 5 attend a daycare, and even fewer families have a nanny, the chapter is not applicable to families that are not upper middle class.
Then again, no book can be all things to all people. What makes Cribsheet shine is Dr. Oster’s writing style. She weaves clinical data with stories about her own parenting journey in a witty, self-deprecating style that makes you feel like you are receiving advice from a wise friend rather than a detached expert. Dr. Oster can’t settle every parenting debate, but it can give you the confidence to make your own decisions when the science runs out – which it turns out, is most of the time.
Now onto a sample of the content of the book.
Breastfeeding
Prior to delivering her daughter, Dr. Oster took a breastfeeding class at a Chicago hospital and was given a list of purported benefits of breastfeeding. One of them was that Mom would form better friendships. She was skeptical and, upon researching it herself, found out that no one had actually researched this topic. But there were some more plausible benefits for breastfeeding. What does the data say?
One problem with studies of breastfeeding is that they tend to be observational studies rather than randomly controlled trials (RCTs). This means that they tend to not control for the fact that women who breastfeed are different from the ones that don’t. For example, studies find that breastfed children have lower rates of diabetes later in life. However, women who breastfeed also have higher incomes than ones that don’t, and poorer children are more likely to develop diabetes. That could mean the poverty causes diabetes rather than breastfeeding preventing it. Once you control for demographics, things like babies who are breastfed having higher IQs tend to disappear.
There is one big randomized controlled trial of breastfeeding called PROBIT that was carried out in Belarus. It found that breastfed infants were less likely to have diarrhea and rashes than infants fed formula. But for many illnesses, the rates that they had them were identical. Some observational studies have found breastfeeding reduces ear infections, such as one in the Netherlands, but other studies in the UK find no relationship.
I personally have heard that breastfeeding is good for the baby’s immune system. But Dr. Oster didn’t cover that in the book, so I don’t know if it’s true or not. But if you decline to breastfeed or can’t, don’t feel that you are setting up your child for failure.
Sleep
Sleep deprivation is one of the most brutal aspects of early parenthood. Those first months can feel like an endless blur of two-hour increments and 3 a.m. feedings. Parents will do a lot to get an uninterrupted few hours of sleep, but will sleep training your baby harm them? How do you best protect your baby from SIDS?
Safe Sleep
SIDS is the leading cause of death in infants in the US, killing around 0.5% of children, almost always in the first four months of life. The causes are poorly understood, but a few interventions have cut down SIDS dramatically.
Intervention 1: Babies on Their Backs!
SIDS, thankfully, is rare, so it’s difficult to study. There has never been an RCT of putting babies to sleep on their backs and relied on case-control studies. However, evidence from these studies was so strong that the American Academy of Pediatrics decided to recommend back sleeping in the absence of a randomized trial. Later studies observing the effects of a “Back to Sleep” campaign in Denmark justified this, finding that deaths from SIDS fell by half in the months after the campaign started, preventing an overall 8% of infant deaths.
Intervention 2: Alone in Their Crib
This recommendation forbids co-sleeping or putting blankets. It’s easy enough to keep stuff out of the crib, especially with the advent of wearable blankets and swaddles. But many infants sleep better with a parent. How risky is co-sleeping?
Co-sleeping in any form is associated with an elevated risk of SIDS. But the level of risk depends on the parent’s behaviors, especially if they smoke or drink. See the following chart:
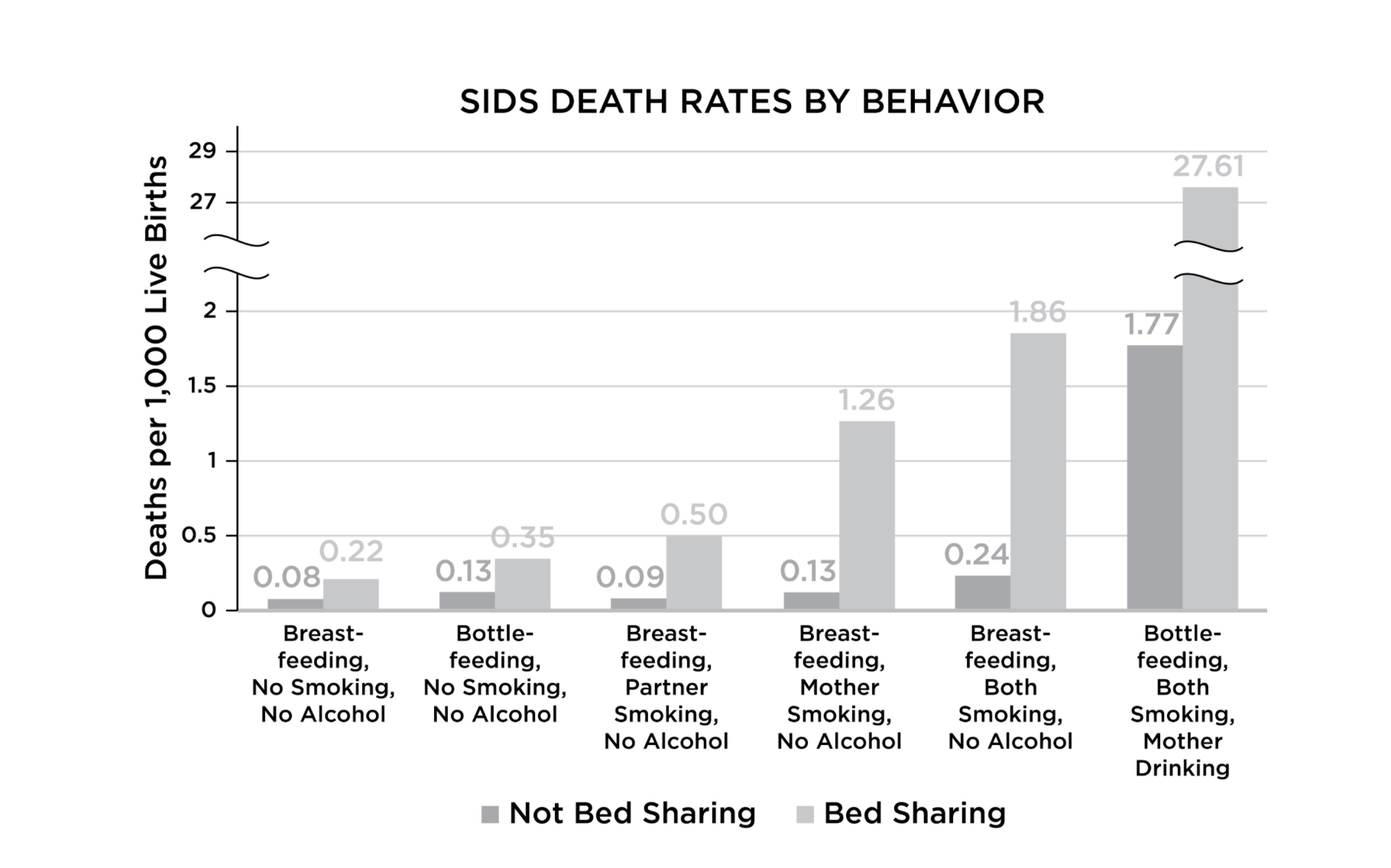
Even more dangerous is sharing a sofa with an infant. Sleeping together on a sofa is 20x to 60x riskier than the baseline rate in the graph.
While the official guidelines are to never co-sleep with an infant, Dr. Oster takes a more moderate position: if it’s the only way your family can get sleep, do it as safely as possible: don’t smoke or drink, put the baby on their back, and take blankets off your bed.
Intervention 3: In the Room with the Parents
This recommendation has the weakest evidence associated with it: the studies done were smaller and not explicitly looking at a relationship between room sharing and SIDS. They tend to be sensitive to which variables are adjusted for and depend on whether the infant was sleeping on their stomach.
At the same time, there is a cost to room sharing: child sleep. By nine months, infants who slept in their own room sleep 45 minutes longer than those who don’t. While the evidence is not causal (parents may move the baby to their own room when they sleep better). Sleep is important for infant brain development, so it’s not just important for the parents.
Intervention 4: No Soft Stuff
As before, blankets and toys should not be in the crib. Dr. Oster looks at the effects of crib bumpers on SIDS. Only one study looked at this and attributed 48 deaths to them between 1985 and 2012, or .007% of all SIDS deaths. She still recommends against having them, as older children can use them to fall out of the crib, but they are negligible in terms of SIDS risk.
Sleep Training
There are people who will tell you their baby slept through the night from three weeks on. In my experienced opinion, most of these people are liars
Infants like to get up a lot; parents would rather not. The marketplace has noticed this, and there is an avalanche of books to get your child to sleep better. All of them promise better sleep and happier parenting, but do they work? And will they stunt your child long-term?
The approaches fall into two broad camps: some form of “cry it out” (the Ferber or Weissbluth methods), and “no-cry” methods that rely on gentler interventions. There are also attachment parenting advocates who argue you shouldn’t be sleep training at all – that leaving babies to cry themselves to sleep damages their emotional development and undermines the parent-child bond.
Two approaches to “cry it out” techniques have received extensive study: “Extinction” (leave the room and don’t return until morning) and “Graduated Extinction” (check on the baby at increasingly lengthy intervals). Across 17 studies on Extinction and 14 on Graduated Extinction, the results were consistent: it works. Sleep-trained babies woke up about half as often during the night each week, and parents who used these methods reported less depression and better mental health.
But is it bad for the baby? There’s little evidence that it is. One rigorous Australian study followed 328 families for five years after sleep training and found no differences in emotional development, behavior problems, or parent-child attachment between the sleep-trained group and those who weren’t sleep trained.
Dr. Oster got a lot of pushback on this chapter from attachment parenting advocates and some developmental psychologists who felt she dismissed their concerns too quickly. They pointed out studies showing infants and mothers had similar cortisol (stress hormone) levels before and during sleep training. Once sleep training had concluded after three days, infants had the same level of cortisol, while mothers had lower cortisol. The researchers interpreted this as a sign the mother-baby bond was deteriorating. Dr. Oster disagrees, saying that nothing happened to the infants and the mothers were more relaxed afterwards, a net benefit.
Vaccines
No discussion of the Mommy Wars would be complete without mentioning vaccines. Distrust of vaccines has spiked recently, and outbreaks of diseases like measles are back in the news. Distrust of vaccines is not exactly new; for example, in India and China there was distrust of the smallpox vaccine. In the late 70s a paper was published linking the DTaP vaccine to infant brain injury. The paper was flawed, but a bunch of lawsuits were filed, prices rose, and availability tanked. Congress passed the National Childhood Vaccine Injury Act in 1986 to shield manufacturers from these lawsuits and stabilize the supply. The most recent round of distrust, however, started with ex-Dr. Andrew Wakefield and a paper linking the MMR vaccine to autism.
With all the distrust of vaccines, what does the data say? In 2011 the Institute of Medicine, now the National Academy of Medicine, released a comprehensive report (Effects of Vaccines: Evidence and Causality) that looked at 12,000 studies looking at 158 different kinds of adverse events to common childhood vaccinations. They drew the evidence from adverse event reports and epidemiological studies and tried to decide if a relationship was there, not there, or not enough evidence to decide. Most of the time, they couldn’t really answer the question either way. There were 17 kinds of adverse events they found a relationship with. 14 of which were supported by the evidence and 3 rejected They can be categorized as follows:
- Allergic reactions
- Fainting, mostly in adolescents
- Things specific to the immunocompromised
- Febrile seizures
Allergic reactions are pretty rare, occurring in only 2.2 per million vaccinations given. Fainting occurs in 3 in 10,000 vaccinations. About 2.5% of children will get them before age 5. Most are not vaccine related, but there is an elevated risk of them up to 10 days after the MMR vaccine. Febrile seizures are linked to high fevers and, while serious, have no long-term effects on children. While there are some risks to vaccines, these are small risks. We routinely take bigger risks every day. At the same time, they are effective at preventing disease. For example, comparisons of children born in the fall versus children born in other parts of the year show that they are more likely to get vaccinated for the flu because their routine doctor’s appointments occur during flu season. The same study found that the vaccinated kids, are less likely to get the flu.
What about spacing out the vaccines more, an increasingly popular option? That actually makes febrile seizures more likely, because that reaction to the MMR vaccine is more common as kids get older than 1 year.
At this point, you’re getting a sense of what each chapter is like; Dr. Oster introduces a common parenting question, finds any study out there related to the topic, and explains what the data says interspersed with humorous anecdotes about her own experiences parenting. It’s a formula that works well, and one I’ll happily follow for a third volume.
There are some limitations on the empirical approaches advocated by this book. Dr. Oster cheerfully notes this in her chapter on screen time, noting that data and studies have little to say on long-term impacts of screen time. That being said, 8 hours of screen time a day would probably have some negative impacts. Sometimes, what you need is common sense, not a randomly controlled trial.
Stray Observations
-
I highly recommend reading this book before your child is born - I was only halfway through the book when our son arrived and didn’t pick it up again until 6 months later. Many of the things I learned in this book would have been useful during this period.
-
A lot of the studies mentioned in this book look at whether certain parenting decisions are related to obesity. Given the advent of GLP-1 agonists, I wonder how many studies will look at obesity rates in the future.
-
Apparently, there are people out there saying that drinking beer improves mothers’ milk supply. I had never heard this before, but drinking alcohol dehydrates, decreasing milk supply. However, there is no evidence supporting pumping and dumping.
-
A lot of the weirder ideas, such as “no cauliflower while breastfeeding” type advice came from the grandparents. I’m glad my mom didn’t say anything crazy to me.
-
After delivering her daughter, Dr. Oster had trouble with breastfeeding. The doctors, to avoid something called “nipple confusion,” (wut?) had some sort of contraption that involved taping a tube to her breast to feed her daughter from the bottle. She declined to bring the device home.
-
Another interesting diversion between empiricism and logic: how to introduce solid foods. The official guidelines are to introduce rice or oatmeal first, then introduce fruit or vegetables, one variety at a time for a few days. This is on the theory that you can mix cereals with breast milk or formula and they’ll be more likely to accept it. You introduce only one variety at a time to control for allergens. These specifics have never been tested. However, Dr. Oster points out that most allergies are caused by peanuts, tree nuts, eggs, and milk. While introducing those foods one at a time makes sense, mixing apples and pears is fine.
-
The guidelines also recommend not to introduce honey before 1 year due to the risk of botulism. While there were some high-profile cases of botulism in the 70s from honey, the actual rate of infant botulism has not changed since the guidelines changed, so maybe its not the driving source of infant botulism.